aspirin, SCDs, TED hose lovenox DVT prophylaxis surgical fasciatomy Pallor sign of arterial insufficiency below level of injury something to reduce risk or hip fracture 85% % of hip fractures in people older than 65 This traction has an external pin distal to stabilized area fascia can't expand to increased pressure Paresthesia decreased sensation, hypersensation - result of nerve compression fat particles lodge in vessel Risk factors for compartment syndrome trauma, plaster cast, ortho postops, burns, infected limb neurovascular assessment focus areas (5Ps) BKA below the knee amputation Pain Worry if this is out proportion to injury - - not relieved by meds age, type of fx, bone quality factors considered for hip fx treatment neurovascular assessment assessing nerve function and blood flow to injured extremity This should never be placed under the knee after TKA ORIF open reduction internal fixation out of bed This should happen on post op day 0 1-3 days after injury (usually femur) when trauma pt will typically develop fat embolism Paralysis Late sign of prolonged nerve compression or muscle necrosis Osteoporosis and falls Risk factors for hip fx Pulse use a doppler if you can't palpate this Early mobilization decreases mortality rate after ortho post op Buck's traction aspirin, SCDs, TED hose lovenox DVT prophylaxis surgical fasciatomy Pallor sign of arterial insufficiency below level of injury something to reduce risk or hip fracture 85% % of hip fractures in people older than 65 This traction has an external pin distal to stabilized area fascia can't expand to increased pressure Paresthesia decreased sensation, hypersensation - result of nerve compression fat particles lodge in vessel Risk factors for compartment syndrome trauma, plaster cast, ortho postops, burns, infected limb neurovascular assessment focus areas (5Ps) BKA below the knee amputation Pain Worry if this is out proportion to injury - - not relieved by meds age, type of fx, bone quality factors considered for hip fx treatment neurovascular assessment assessing nerve function and blood flow to injured extremity This should never be placed under the knee after TKA ORIF open reduction internal fixation out of bed This should happen on post op day 0 1-3 days after injury (usually femur) when trauma pt will typically develop fat embolism Paralysis Late sign of prolonged nerve compression or muscle necrosis Osteoporosis and falls Risk factors for hip fx Pulse use a doppler if you can't palpate this Early mobilization decreases mortality rate after ortho post op Buck's traction
(Print)
O-DVT prophylaxis
O-surgical fasciatomy
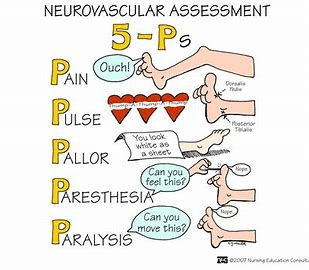
G-sign of arterial insufficiency below level of injury
O-something to reduce risk or hip fracture
N-% of hip fractures in people older than 65
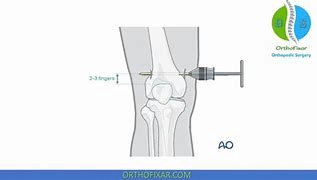
N-This traction has an external pin distal to stabilized area
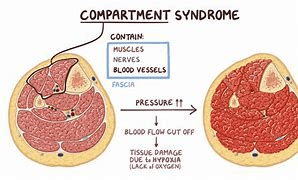
B-fascia can't expand to increased pressure
I-decreased sensation, hypersensation - result of nerve compression
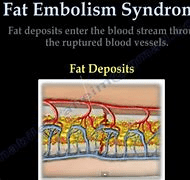
B-fat particles lodge in vessel
B-trauma, plaster cast, ortho postops, burns, infected limb
I-neurovascular assessment focus areas (5Ps)
I-below the knee amputation
N-Worry if this is out proportion to injury - - not relieved by meds
B-factors considered for hip fx treatment
O-assessing nerve function and blood flow to injured extremity
G-This should never be placed under the knee after TKA
I-open reduction internal fixation
O-This should happen on post op day 0
G-when trauma pt will typically develop fat embolism
N-Late sign of prolonged nerve compression or muscle necrosis
B-Risk factors for hip fx
G-use a doppler if you can't palpate this
I-decreases mortality rate after ortho post op
G-Buck's traction